An anal abscess results when a perianal gland becomes infected. It causes severe pain in the region around the anus. There may also be discharge of pus or blood from the anus with an offensive odour.
Types
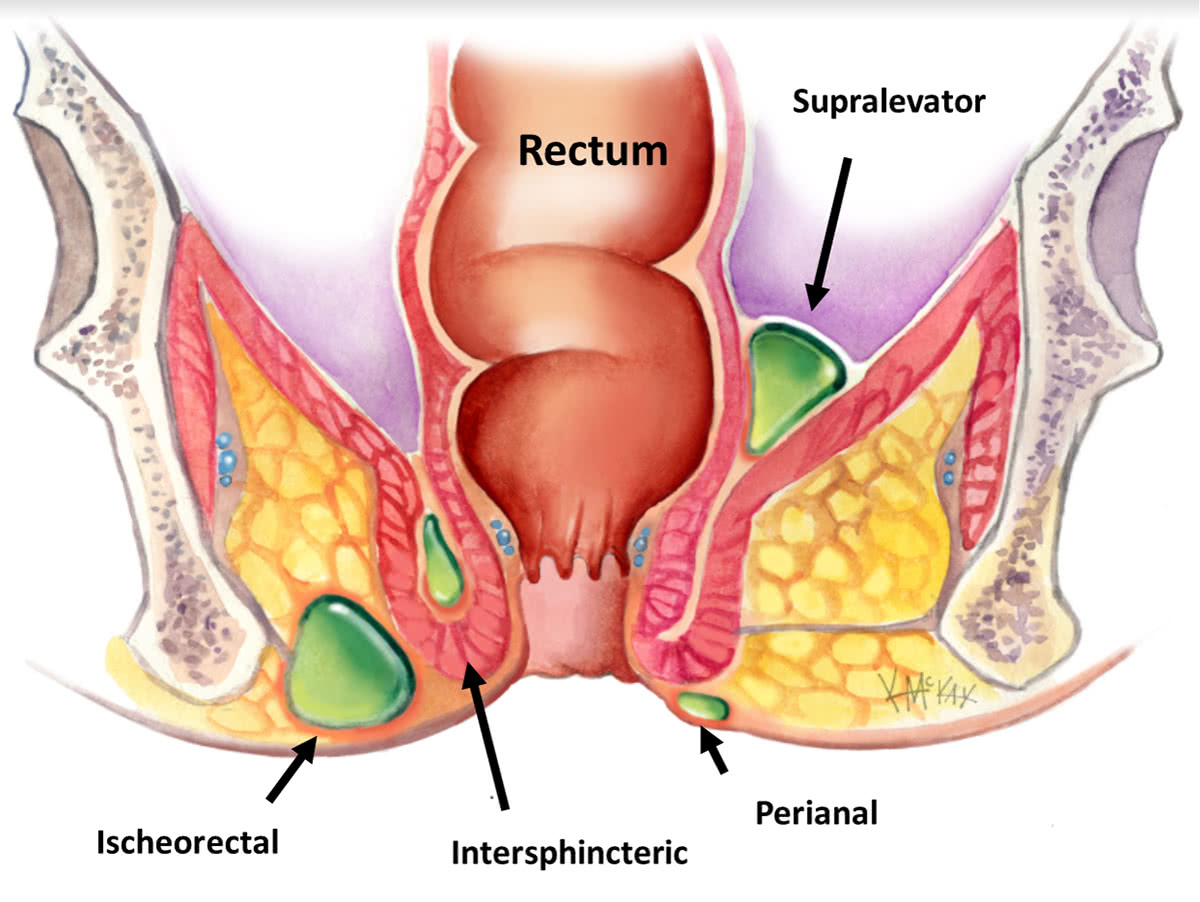
Perianal abscesses can be small and localised to the anal region (perianal abscess), be confined to the space between the internal and external anal sphincter (intersphincteric abscess), be large extending into the buttock region (ischiorectal), or rarely be high above the muscular floor of the pelvis (supralevator abscess).
Cause
Most abscesses result from infection of one of 15-20 perianal glands located in the anal canal (Cryptoglandular hypothesis). This is more common in young adults, but can occur at any age. The reason why some people develop it, and others don’t is not known. A less common cause of perianal abscess common in smokers is Hidradenitits suppurativa, Crohn’s Disease is occasionally the cause of a perianal abscess resulting from an anal fistula.
Symptoms
Pain, swelling, redness and discharge of mal-odorous pus from the perianal region are classical signs.
Investigation
The diagnosis is made clinically, and confirmed by an Examination Under Anaesthesia (EUA), where the abscess is also drained.
Course
Over half of perianal abscesses will never recur once incised and drained. Some develop an anal fistula which is a communication between the internal anus and the external skin. If an anal fistula develops it may require further surgery or the insertion of a silastic seton. This is like a rubber band that allows the abscess drainage site to remain open to allow it to drain properly until the inflammation and infection has resolved.
Surgical management
Incision and drainage (lancing) under anaesthesia is the treatment for an acute perianal abscess. Antibiotics for a period of time may also be needed.
What to expect pre and post operatively following anal abscess surgery
Fasting and Bowel Preparation
Unless you are also having a colonoscopy, a normal diet without a bowel prep, is required the day before surgery. You need to fast from midnight the night before if your surgery is scheduled for the morning, or from 7am if scheduled for the afternoon. You will be admitted as a day-stay procedure. You will receive a Fleet® enema 1 hour prior to your operation.
Recovery and transport
Following your procedure, you will recover for an hour until the effects of sedatives have worn off. You should not drive yourself home after your procedure and should have someone organised (a friend or relative) to accompany you.
Bleeding
Spotting of blood or persistent minor oozing will occur for 5 days following your procedure, and a sanitary napkin changed once to twice daily will be needed to prevent staining of your underwear. Bleeding will typically occur after opening your bowels. If the bleeding is more than a couple of teaspoons a day, notify your surgeon.
Laxatives
You should remain on regular laxatives and simple analgesics for 1 week. A tablespoon of natural psyllium husk (Metamucil® or Fibogel®) twice daily, and 30ml of lactulose (Duphalac®) once to twice daily is recommended.
Pain control
For pain, a non-steroidal is recommended such as 400mg of ibuprofen (Brufen®) along with 2 tablets of paracetamol. This should be taken regularly three times a day for five days. Opioid medications (Endone) may sometimes be needed, but should be used sparingly as they cause constipation.
Antibiotics
After discharge from hospital you may require antibiotics to treat ongoing infection. Oral cephazolon (Keflex®) and Metronidazole (Flagyl®) may be needed for 5 days (provided no allergies exist).
Dressings
Occasionally you may be sent home for daily dressings for up to a week, which is often performed by a community nurse or your local general practitioner. If an anal fistula was found at the time of the incision and drainage procedure, then you will be sent home with a silastic seton in place. This is about the size and consistency of a rubber band and is passed through the tract of the fistula to allow ongoing drainage of the abscess.
Sitz baths
Twice daily warm to hot salt water (Sitz) bathing to the anal region is soothing and antiseptic, and should be done for 1 week following your procedure. Put a handful of salt into a shallow bath of warm-to-hot water and sit there for 10-15 minutes.
Follow-up
You should follow up with your colorectal surgeon in 6-8 weeks following your surgery to review your wound and discuss further management if indicated.
