Groin hernias can be repaired as a day-stay procedure using an open or key-hole (laparoscopic) approach. Open repair can be performed under local anaesthetic with sedation, whereas key-hole (laparoscopic) repair requires a general anaesthetic.
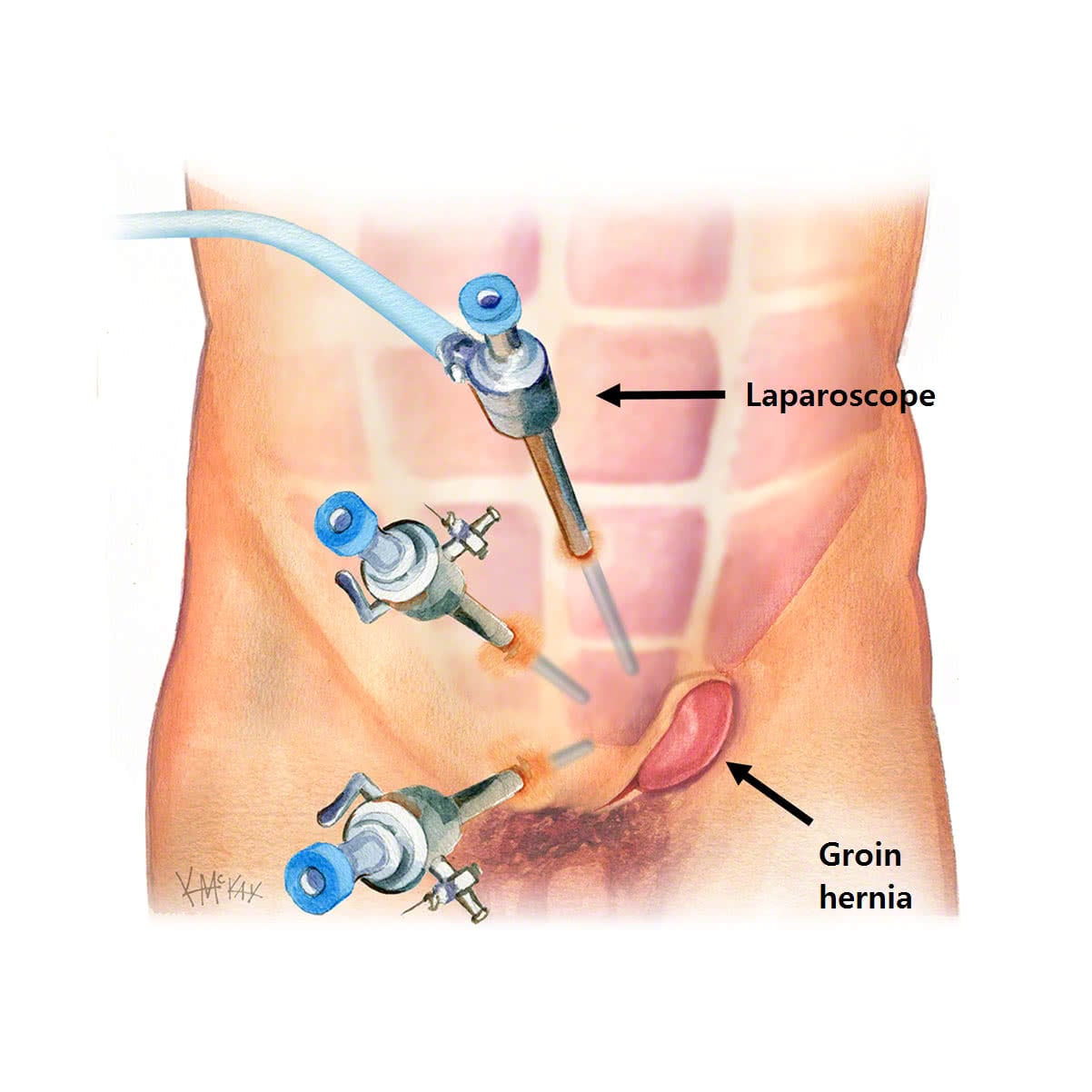
Key-hole (laparoscopic) hernia repair
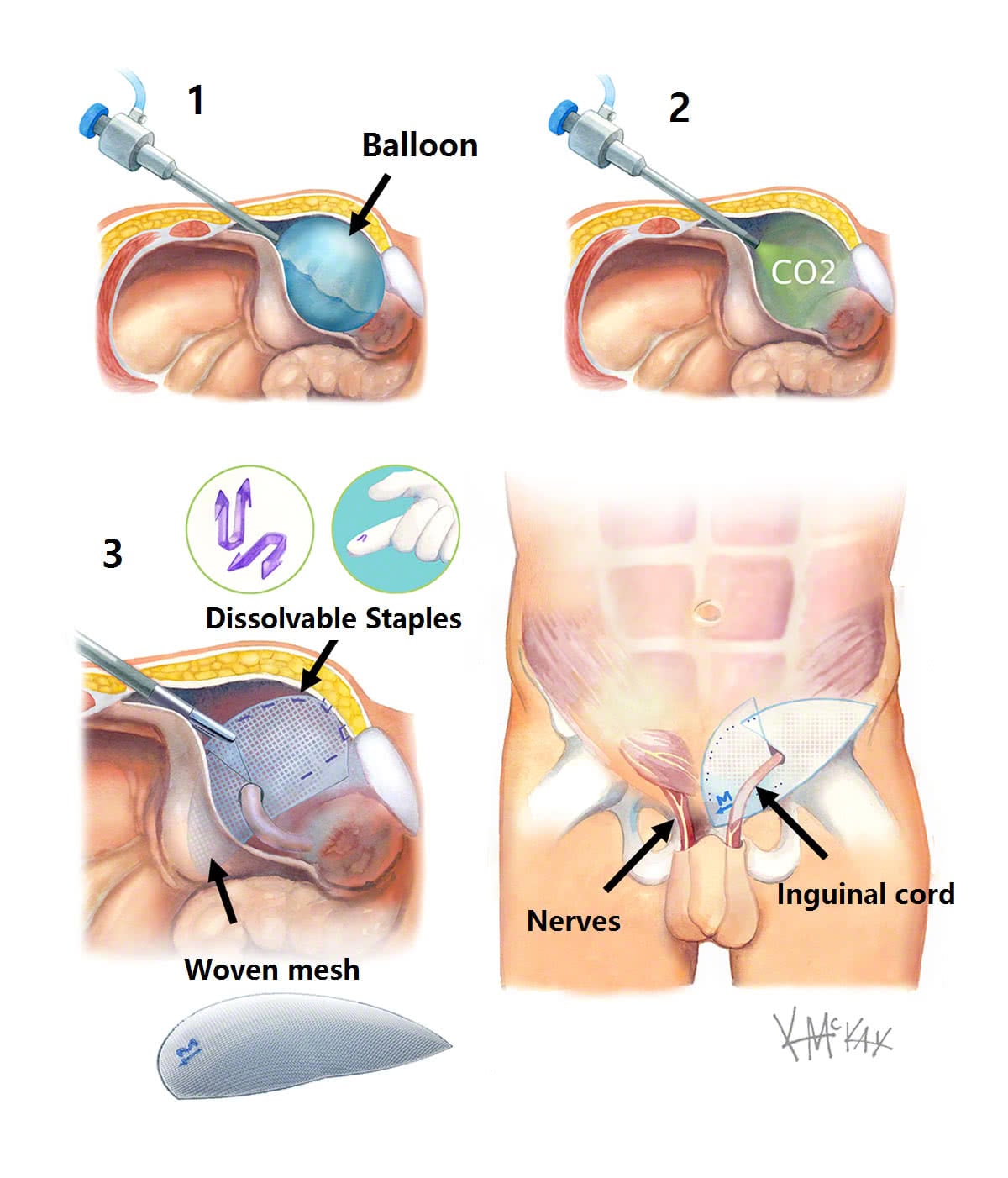
This involves removing the hernia and reinforcing the abdominal wall with the insertion of a custom-designed (Bard 3D®) polypropylene mesh that is secured with dissolvable (Securestrap®) staples. It is achieved with 3 small incisions less than a centimetre in size.
Key-hole (laparoscopic) hernia repair results in less pain than open surgery, allowing for earlier return to usual activities including work.
Why repair hernias?
Hernias will only ever get bigger with time. Elective repair is much easier and safer than emergency repair, and can be done with a key-hole (laparoscopic) approach. If a hernia is not operated on, there is a small chance of bowel getting caught in a hernia, and sometimes this can get stuck (incarcerated) or twisted blocking off the blood supply to the bowel (strangulation). This is a surgical emergency that can result in the need for major surgery including bowel resection.
Risks of hernia repair
There is a 1% risk of hernia recurrence with mesh repair. This risk is further reduced by the avoidance of any heavy lifting (greater than 10kg) in the first 4 weeks following your hernia repair.
There is up to a 5-10% risk of pain lasting more than a week following hernia repair and this is largely due to initial inflammation due to the presence of foreign material (mesh). A combination of simple anaelgesics such as paracetamol and a nonsteroidal such as ibuprofen can help reduce post-operative pain. If the pain lasts more than a week, notify your surgeon immediately, as chronic nerve-type (neuropathic) pain can be avoided by the administration of a nerve block to the groin and the commencement on special atypical pain killers such a nortryptyline (Pamelor®) 25-50mg daily and/or gabapentin (Pregabaline®) 25mg twice daily. These drugs both block neuropathic pain.
Bruising of the scrotal region is common after inguinal hernia surgery. Tight scrotal support (2 pairs of small underpants) in the first week after your surgery can reduce the risk of swelling and bruising to the scrotal region. Occasionally a large bruise or collection of blood (haematoma) develops. If this occurs, you should contact your surgeon immediately.
Testicular injury is a rare but serious complication of hernia repair. Hernia repair involves removing a hernial sac from the blood supply (testicular artery) and venous drainage (pampiniform plexus) of the testicle, as well as the spermatic cord (vas deferens). The risk of injury to these vital structures with risk of damage or even loss of testicle is less than 1:1000, except in cases of recurrent hernia surgery where the risk is considerably higher.
What to expect post operatively after key-hole groin hernia surgery
Key-hole (laparoscopic) groin hernia surgery can be performed as a day stay procedure. Following your hernia repair, you will recover for a hour until the effects of the sedatives have worn off. Usually you will be allowed to go home the same day or the very next day. You should not drive yourself home after your procedure and should have someone organised (a friend or relative) to accompany you.
Whilst return to light activities is possible within a few days of key-hole hernia surgery, no heavy lifting (>10kg) should occur for at least 4 weeks following your surgery to avoid a recurrence of your hernia. Simple over the counter analgesia is usually sufficient for pain in the first few days following your surgery.
Your outer (comfeel) dressings can be removed day 7 after your operation, and the inner dressings (steristrips) may be allowed to fall or peeled off day 7-14 after your operation. Your sutures are dissolvable so do not require removing.
You should follow up with your surgeon in 4-6 weeks to review your wound.
